
This is a scary position I am going to take. Contradicting someone of Dr. Brian Vartabedian’s stature is bound to have some repercussions: I hope they are not too profound! Also, hat tip to the awesom @scanman for coming up with the “storm in a tweetcup” comment. I am using it!
Anyways. So here goes nothing!
I am an ardent fan of 33 Charts, which is, undoubtedly, one of the best medical blogs around. But today, he posted something which I had to disagree on. Before I lunge into the reply, here take a look at the following sample of tweets (read last one first – twitter chronology):


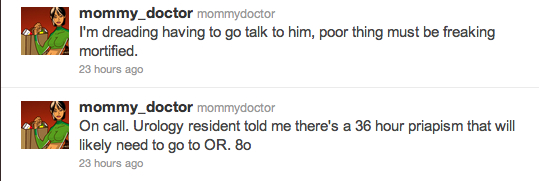
So, Dr. V believes that this constituted unprofessional behavior and vents his ire on his blog. I was surprised to see a lot of people actually go on a witch hunting expedition of @mommy_doctor on this issue. I have no clue of she has had any past history, as has been suggested, because I started following her just after Dr. V helped her to shoot to fame. So, I will consider everything around this post series that Dr. V has taken the arms up against.
1. HIPAA Compliance:
First things first: if you are going to quote it like the Bible, please try to spell it correctly first! The misspellings in the comments section drove me crazy!

(Hat tip: Fizzzy)
She claims to anonymize her patients, and protect their identities, and there may not actually even have been such a case, so this argument falls flat on its face. Dr.V actually concedes that there may not have been any violations in this exchange.
2. Tone of the Discussion:
I agree somewhat with Dr. V on this point. There may have been a bit of an irreverent, if playful tone in that matter, but I don’t think it would be anything super-bad about it. Medical humor, by itself, is dark. Look at what Des Spence has to say in a short article that touched the core of this issue:
I remember bursting through the doors to the hospital doctors’ mess to the sound of loud, repeated, almost stuttering swearing. Swearing was ubiquitous in theatre, in emergency departments, on ward rounds—under my breath, in my head, in my dreams. Swearing even has it own universal sign language. Swearing is an intrigue, part of the medical training and tradition. Indeed, if I could translate ancient Greek I would be surprised if swearing wasn’t part of the original version of the Hippocratic oath. Even those doctors who didn’t enjoy smoking and those with strong religious convictions enjoyed a good swear at 3 am during medical receiving.
This workplace swearing—unnecessary, loud, wanton, gratuitous, unprofessional, and, the very point of it all, therapeutic—is not to be confused with the aggressive swearing of personal attacks. It may not be big and not clever, but it is a highly effective stress buster and indeed strangely attractive, endearing, and often supremely funny.
On the best of days, we work through blood, gore and death, and if someone finds a little catharsis in a little dark humor, is it justified to take up the cudgels against them?
I am absolutely nauseated by the people who say that this is an inappropriate thing to say in public. What they mean is that it is alright if discussed privately, behind closed doors, as Des would say… this hypocrisy is what I abhor. If it is inappropriate in public, it is inappropriate behind closed doors as well. Just because the patient *may* not come across the closeted ramblings does not make that any lesser a crime (working on the assertion that it is a crime, that is).
3. Anonymity:
Well, this is another thing I feel strongly about. When I started off blogging on this site in November/December 2010, I started off anonymously. Having had a bad experience with my previous blog on account of my stand on issues like politics, sexuality and caste-based reservations, I was wary when I started this blog. But soon enough, I realized as long as I do not lend a face and a name to the content, there is not going to be any credibility. Accordingly, I came out. And since then, the interaction and chatter on my blog has gone up markedly.
Also, I agree with Dr. V when he says a lot of people hide behind the façade of anonymity to vent unjustified ire over the internet.
4. Lack of Compassion:
Seriously, Dr. V, you think if we indulge in a bit of bantering, we are compromising on compassion? If anything, in my very, very limited personal clinical experience, I have seen a sense of humor goes a long way in comforting the patients and their families. Also, she shows her compassionate side when she says she would not let the man suffer from such prolonged pain had it been up to her. (please do remember the context: this was not per se her opinion of “managing” the patient – she was just replying to someone who was flirting with her!)
5. The Medical Issue:
Some of the commenters have raised the valid question that maybe bantering around the tumescence of any other organ would not have resulted in this post. 33 charts has been one of my staple reads and I have found Dr. V’s style to be very logical and enjoyable. I would like to believe that he did not single out this issue because of the priapism and was just pissed at the whole conversation…
6. Making mountains out of molehills:
Apparently the American health system is very good at it. That is why they spend billions managing lawsuits every year.
7. Discussing patients:
If the twitter bio is truthful, a lot of details have been changed, or maybe even the patients is fictionalized. Heck, we are not even sure is @mommy-doctor is a real doctor or a llama herder (as one commenter remarked). When the whole thing is so nebulous, I think the better thing to do is just enjoy the dark humor, or pass it up if its too much for you!
[On another note, I wonder what would happen to Dr. V if he were reading the #penisfriday posts @burbdoc posts! His head might explode!]
In conclusion:
I find nothing to make such a hue and cry over this matter. It is probably a better idea to play it safe and not say anything that can get misinterpreted, but then again, if you are going to say something useful, from time to time, people are going to misinterpret you.
Overall, I think he over reacted a bit to this issue (as am I by writing this huge blog post in rebuttal!) and it is hard to believe that this is the same person who, just a few days ago, wrote this:
And do we really need to announce that our shared links don’t represent endorsement? Who in the free world really thinks that when I retweet a link or idea I’m formally endorsing the site on the receiving end? When was the last time a shared link lead to identifiable damages from the lack of the endorsement disclaimer?
I can understand disclaimers about medical advice. But we’re all waiting for that first big judgment against the ‘disclaimerless’ doctor brought to her knees by that loose tweet construed by the patient-victim as individual medical advice. Rest assured that when it happens you’ll hear it here first.
Ultimately I think this use of language is about fear. But I suspect that those interested in getting at us won’t be deterred by cut-and-paste disclaimers. Perhaps it’s time to rethink the practical utility of the disclaimer.

Dear recent medical graduate, the sad reality is that whether you are in the grocery store, Starbucks, jogging around your neighborhood or posting/tweeting/blogging anonymously as a “physician” on the Internet, you are representing the medical profession. Your buddies and those with similar sensibilities may think the humor is cool. I explain that fact to my 19 and 24 year old nieces. I also explain that current and future employers may not think it is cool (just like their frumpy aunt.)
In the realm of medical professionals posting/tweeting/blogging we (the patients) are also your audience. And, with all frankness, if you don’t take your profession seriously, neither will the patients. That translates into patients thinking: (1) medicine should be a right and they should get all medical care for free; (2) physicians deserve to be sued because they are jerks anyway; (3) physicians do not care about patients (and therefore why should we pay them and why not sue them if the outcome is not 100%).
I suggest that you act in areas of you public life as you want us (the patients, your professional medical colleagues and potential medical referrals and employers) to treat you.
LikeLike
So basically what you are saying is that as doctors, we should mould our conduct in order to facilitate the often times illogical behavior of patients? That literally makes no sense. You are asking us to be hypocrites, in effect…
LikeLike
You say:
“I am absolutely nauseated by the people who say that this is an inappropriate thing to say in public. What they mean is that it is alright if discussed privately, behind closed doors, as Des would say… this hypocrisy is what I abhor.”
You totally miss the point. There’s a HUGE difference between venting to your coworkers as a way of dealing with work stress, vs announcing a patient’s condition for the amusement of everyone on Twitter, and therefore to the rest of the world. Scale matters in the degree of damage, you can’t ignore that.
Second, you can’t rule out HIPAA violation. How many 36h priapism patients were seen by a female Asian anesthesiologist on 5/23? This info is available on @mommy_doctor’s Twitter profile, and is reasonably identifiable. Besides, the patient can recognize himself. This definitely is unprofessional behavior and is grossly harmful to the patient’s dignity.
Lastly, remember the Rhode Island ER doc who got fired for posting on FaceBook about a patient’s condition, even tho she “anonymized the patient” – the patient recognized himself and was offended, and she was fired. Rightly so, because she violated the patient’s trust and did some damage. Here’s the link on KevinMD: http://tinyurl.com/3e7wbpq
LikeLike
Just to add, when she said:
“I’m not that mean – would’ve fished or cut bait by now”
That’s a sexual innuendo. Meaning she would have “relieved” the patient’s boner or left him alone, if she was in fact causing his erection. That’s WRONG coming from a physician. Don’t defend that.
LikeLike
1. If you can’t vent, you can’t vent to anyone. Scale should not be an issue. You can get your patient identity compromised by talking to 5 or 5000 people – in either cases you are guilty. Equally guilty. Don’t get me wrong – discussing cases is a dicey affair, I agree, but as far as the philosophy of the thing goes, scale should not be a consideration.
2. Are you sure the patient existed? What if she conjured the patient and then made the innuendo? Then, by extension of your logic, I could say that if I made a patient up, I could do anything with them! Hey, if you don’t exist, you can’t get offended, right?
3. I remember reading that, and then then the story of a nursing student who clicked placenta pics and got thrown out, then sued and won. There are stories and counter stories. Again, by this same logic, Dr. V is more guilty (scale and all) since his blogging the issue took it to a whole different level altogether! (I guess I am guilty by extension too!)
LikeLike
The boner was the issue of his chagrin, so by relieving it however, she was doing him a favor, isn’t it?
Humor alert: Don’t go about suing me now! 🙂
LikeLike
It’s not me you should be worried about. Let’s hope your patients share your sense of humor.
LikeLike
As a patient who has a good sense of humor, I would be offended if I recognized myself in my doctor’s tweets. I would also report him or her to his or her hospital, practice privacy officer, state medical board, specialty society and the Office of Civil Rights (which is where you file official complaints for HIPAA violations).
What you’re talking about may be humor in your mind and, perhaps, even in the minds of some of your colleagues, but it is NOT humor in the minds of many (if not most) patients who seek your help and trust you… even those who are known for having a great sense of humor.
Go ahead and keep up this “humor,” but if you’re trying to avoid being a hypocrite, don’t ever utter a word about how little patients trust doctors these days… or how little the public respects the medical profession these days… or how your profession continues to lose prestige… these days. You can’t have it both ways. You respect the patients or you don’t. But the patients pay for the roof over your head and the public (patients) confer respect and prestige upon your profession (or they choose not to). Do what you want… just acknowledge the consequences and the people you may hurt (including yourself and your colleagues).
LikeLike
Would you be this offended if the issue at hand was not an extended erection, but, say, cramping abdominal pain?
LikeLike
Pranab, I think patients would be more offended/hurt if we joked about his penis, rather than stomach pain. And because that difference matters to our patients, wit should matter to physicians as well.
It’s tempting to argue this in black or white terms, to say that all such discussions are either OK or not OK, regardless of which body parts. But it’s not so simple when part of our duty is to protect the patient’s emotional well being.
LikeLike
Somehow, as a doctor, I fail to see why all our communications are necessarily interpreted as being of a professional nature, even if one is reading them off a decidedly impersonal and unrelated platform like, say, social networking sites or blogs.
I have as much right as the next man to be a foul mouthed racist/casteist/religiously bigoted pig on the platform of my choice, as long as it is not in my consulting chamber or operating room, where the poor dear on the couch might get nervous.
We’re not politicians. We’re not Paris Hilton. We’re not industrialists. Get off our backs!
And we’re not CIA either. We can talk about our work online. If the identity of the patient in question is not exposed, I fail to see how it is unethical.
LikeLike
As person, you have a right to say what you want, but only when you say it as John Smith. When you say it as Dr. Smith, you are representing all of us as doctors. Whether you like or not, as a doctor, you are part of a profession and and a community. While free speech still applies, things you say and do as a doctor, impact how others see ALL of us, not just you as the individual.
LikeLike
“I am absolutely nauseated by the people who say that this is an inappropriate thing to say in public… If it is inappropriate in public, it is inappropriate behind closed doors as well.”
I would strongly disagree. Clearly there is a difference between the two, both on a personal and professional level. Every job, not just medicine, has an element of black humor. Its how we as humans, as social beings, cope with things with find unpleasant. We talk about it. We need to. We have to. But we also need to be aware of the appropriate times and places to do it.
LikeLike
Hi Pranab, I ran across your blog following the storm in a tweetcup. I am not a physician. I wrote about my response at Anonymity, pseudonymity, privacy, online discussions, and deleting posted materials, and linked to your blog.
Salient point here: I think Dr. Vartabedian fails to make an important distinction between anonymity & pseudonymity.
A point I did not address but that doesn’t mean it isn’t pertinent: the gender issues. Here a female physician was commenting on a putative male patient’s sexual condition (specifically, the as-it-turns-out-imaginary priapism) — well, let me just say that if a male physician had posted a tweet about attending a female patient who had been unable to urinate for >24 hours, the whole thing would have just been ignored.
LikeLike
If I found out you were talking to me on Twitter even if you were completely protecting my anonymity, I sure as hell will not come back to you.
LikeLike